Nursing Diagnosis
Subject: Fundamentals of Nursing

Overview
A clinical assessment of a person's, family's, and community's reactions to an actual or potential health condition may be used to make a nursing diagnosis as part of the nursing process. It is the recognition of the nursing issues with the patient.
"A nursing diagnosis is a clinical judgment about an individual, family or community responses to actual or potential diagnosis provide the basis for selection of nursing interventions to achieve outcomes for which the nurse is accountable." NANDA, 2009. eidam
A nurse acquires the data necessary to draw diagnostic findings regarding the patient's care during the nursing evaluation procedure. The second phase in the nursing process and result of the nursing assessment is the nursing diagnosis. The correctness of the nursing diagnosis determines how effective any intervention will be. The nurse needs to be aware of the data to gather in order to develop an appropriate nursing diagnosis. The conclusion is derived through a critical examination of the assessment data. There are various benefits to using formal, standard nursing diagnostic statements in nursing practice.
- Gives nurses and other members of the healthcare team a common language to comprehend the patient's needs by providing a specific definition of the patient's problem.
- Enables nurses to effectively communicate with other healthcare professionals, the public, and themselves about people's requirements for healthcare and what they do to meet those needs.
- Distinguishes the job of the nurse from that of the doctor or other medical professional.
- Aids nurses in concentrating on the range of nursing practice
- Encourages the growth of nursing knowledge
- Encourages the development of practice guidelines that capture the spirit of nursing
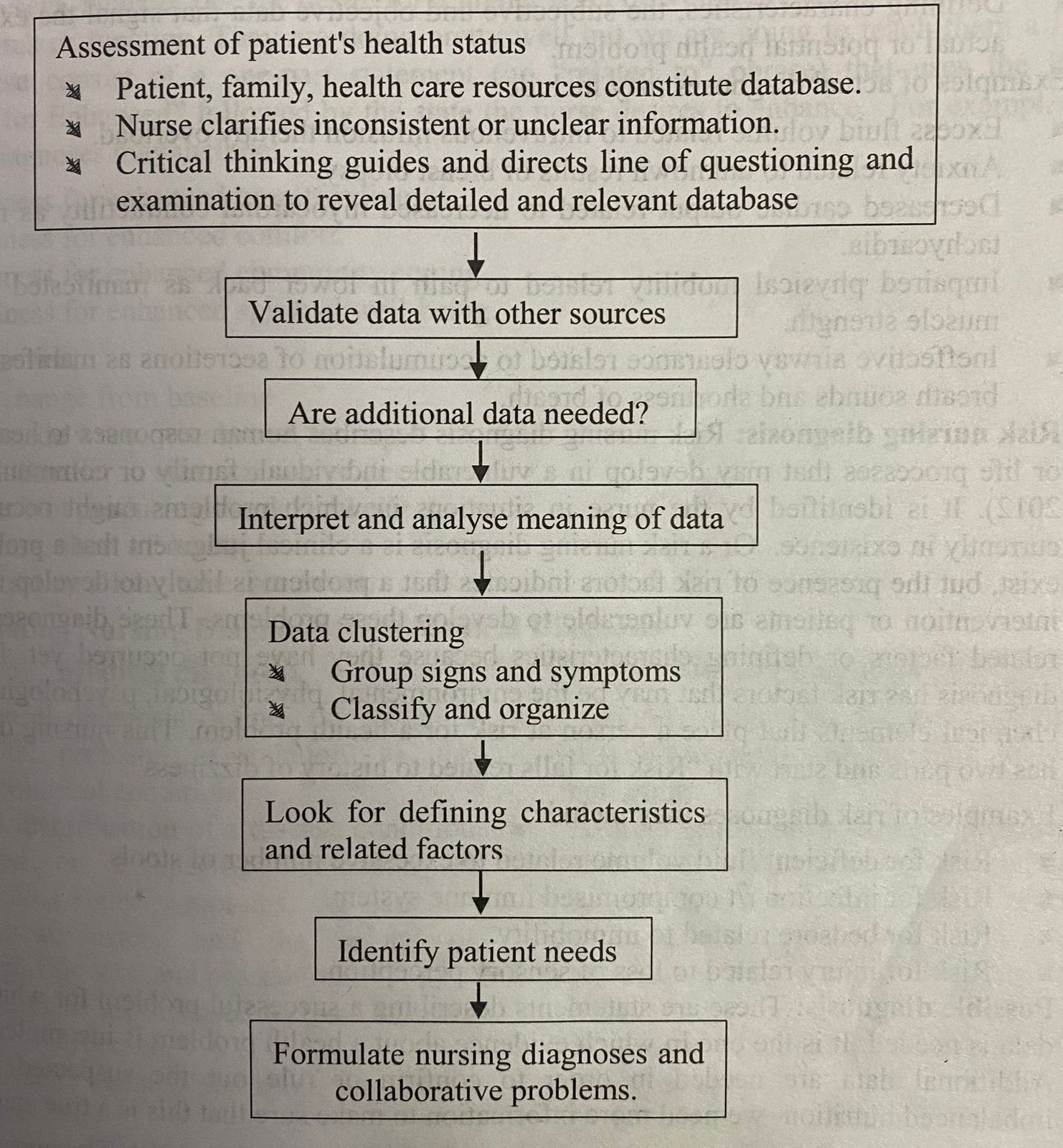
The assessment phase feeds into the diagnostic procedure, which also include decision-making steps. These actions comprise
- Carrying out a nursing evaluation
- Data clustering
- Finding patient health issues
- Diagnosing the condition.
A data cluster is a collection of symptoms and indicators acquired during assessment that make sense when they are grouped together. Data clusters are collections of data that have distinguishing traits or clinical standards that may be observed and confirmed. Each clinical criterion consists of an objective subjective sign, symptom, or risk factor that, when examined in conjunction with other criterion, results in a diagnosis. You start to think about the patients' health issues as you analyze groups of data. The information can be interpreted to enable choosing the appropriate diagnoses from a range of possibilities. The right diagnostic label must be chosen in order to meet a patient's needs. Typically, information progresses from general to specific from assessment to diagnosis.
Types of Nursing Diagnosis
Five groups can be used to categorize nursing diagnoses: actual, risk, potential, syndrome, and wellbeing. Actual and danger diagnoses are the most typical nursing diagnosis. NANDA approved wellness diagnostics in 1996, and Carpenito (1995) discussed potential nursing diagnoses.
Actual nursing diagnosis
- An accurate nursing diagnosis reflects how people react to health issues or underlying life processes in a person, family, or community. Defining traits assist the diagnostic assessment (NANDA, 2012). At the time of the nursing evaluation, the issue is one that the client is experiencing. The presence of corresponding signs and symptoms serves as the foundation for a nursing diagnosis. These issues that the nurse identified are already present. This three-part nursing diagnosiss.
- Give as much detail as you can about the client's health condition or issue, including the root reason.
- Do not utilize medical diagnosis; instead, identify the etiological factors thought to be connected to the issue as a cause or contributing factor.
- Characteristics, both subjective and objective, that indicate the presence of a real or potential health issue.
Actual diagnoses include, for example
- A surplus of fluid brought on by intravenous infusion therapy overload.
- Anxiety at the breast biopsy's potential outcomes.
- Decreased myocardial contractility, which is reflected in tachycardia, and lower cardiac output.
- Reduced muscle strength and reduced physical mobility as a result of lower back discomfort.
- Shortness of breath and changed breath sounds are signs of ineffective airway clearance caused by secretion buildup.
Risk nursing diagnosis
- Risk nursing diagnosis explains how people react to health issues or natural processes that could arise in a weak person, family, or community (NANDA, 2012). The nurse will spot it in circumstances where issues could arise but aren't currently present. A risk nursing diagnosis, on the other hand, is a clinical determination that a problem does not exist, but the existence of risk factors suggests that a problem is likely to arise absent nurse intervention or patients who are predisposed to these difficulties. Because they haven't happened yet, these diagnoses don't have any identifying traits or linked variables.Instead, a risk diagnosis identifies factors that increase a person's likelihood of developing a health issue. These factors can be environmental, physiological, psychological, genetic, or chemical in nature. There are only two sections to this nursing diagnostic, which begins with "Risk for falls due to history of dizziness."
Risk diagnoses can include, for instance
- Risk of inadequate fluid volume due to an abundance of stools.
- Infection risk due to weakened immune system.
- Bedsore risk associated with inactivity.
- Injury risk associated with a loss of sensory perception
Possible diagnosis
- These are claims reporting a solved issue for which more information is required. It is the situation where there is insufficient or ambiguous evidence regarding a health issue. We need more information to determine whether the suspected issue, such as nutritional imbalance, is real before we can confirm or rule it out.
Example
- A sick widowed elderly woman who lives alone is brought into the hospital. The nurse observes that she has no visitors and appreciates the nursing staff's interest in and chat with her. The nurse may write a nursing diagnostic of "Possible social isolation related to uncertain etiology" until more information is gathered.
- Potential stress incontinence due to delivery-related tissue trauma.
- Possible worry brought on by marital loss.
Syndrome diagnosis
It is a diagnosis that is connected to a group of actual risk diagnoses that occur concurrently and are best treated as a group through similar interventions and are anticipated to be present as a result of a specific occurrence or circumstance. For instance, the post-traumatic stress disorder, the disuse syndrome, and the relocation stress disorder.
Wellness diagnosis/health promotion
- A professional assessment of an individual's, family's, or community's motivation, desire, and preparedness to improve well-being and realize human health potential as indicated in their willingness to improve certain health behaviors like nutrition and exercise is known as a wellness diagnosis (NANDA, 2012). It identifies the specific or general condition or state that health-promoting actions may improve. There must be two cues. First, a desire for greater wellbeing, followed by a functional present condition or function.They are doing fairly well, but we will give them a little extra instruction. These consist of a one-part statement that uses the label "Potential for Enhanced" followed by the state the nurse wants to improve. There is no "related to" term in these. As illustrations of possible wellness diagnosis, consider:
- Ability to improve breastfeeding.
- Ability to experience improved spiritual wellbeing.
NANDA Levels
An exception to the rule
- Impaired
- Worsened, diminished, or damaged
- Decreased
- Smaller in size, quantity, or intensity.
- Ineffective
- Not bringing about the desired results,
- Acute
- Severe and fleeting in duration
- Chronic
- Long-lasting and recurring
Recognizing the differences between medical and nursing diagnoses
| Medical diagnosis | Nursing diagnosis |
|
|
Components of a NANDA Nursing Diagnosis
- Diagnostic Level
- The nursing diagnosis as recognized by NANDA is known as the diagnostics level. In as few words as possible, it captures the essence of a patient's reaction to medical problems. There are definitions for each and every NANDA-I authorized diagnostic. The definition details the traits of the discovered human response. The diagnostic levels include adjectives that give the diagnosis extra context. As an illustration, the diagnostic of impaired physical mobility uses the adjective impaired to explain the type of mobility or mobility change that best captures the patient's reaction. Compromise, diminished, deficient, delayed, effective, imbalanced, impaired, and elevated are some examples of other descriptions.
- Etiology/related factors
- The relevant factors are found in the patient's assessment data and are the cause of the nursing diagnostic that the patient is presenting. The factors thought to be connected to or causing the detected issue are reflected in the etiology. Specific nursing actions can alter the connected elements, which are linked to a patient's current or probable reaction to the health issue. This means that the etiology identified physiological [such as incision pain] and psychological [such as a fear of losing control] factors. Spiritual [conflict between beliefs and recommended medical procedure], social [inability to speak English], maturational, and environmental or situational. Excessive noise is one example of a factor that is seen to be associated to difficulties as a root cause or a contributing factor. When the diagnosis is made, the problem's etiology and relationship to "cause" and "effect" are indicated by the phrase "related to [R/T]" It always falls under the purview of nursing practice. Sometimes medical diagnoses are listed as the reason of the nursing diagnostic by health care practitioners, which is erroneous because nursing actions do not alter a medical diagnosis. "Acute pain associated to Prostactomy," for instance. It is untrue since nursing interventions have no bearing on the medical determination of whether the prostate gland should be surgically removed. Nursing interventions aimed at adequate wound care, using turning methods to relieve stress on the suture line, and providing non-pharmacological comfort measures are brought about by rewording the diagnostic as "acute pain associated to trauma of incision."
- Defining characteristics
- The existence of a specific diagnostic label is indicated by the cluster of signs and symptoms. The client's signs and symptoms serve as the defining characteristics for true nursing diagnoses. There are no subjective or objective signs to support a risk nursing diagnosis.
Nursing Diagnostic Statements Formulation
Nursing diagnosis statements have been written in a variety of formats. The two-part and three-part statements are two formats that are often used in nursing literature.
- PES format
- A diagnosis becomes even more patient-specific using this method.
- P (problem)
- The client's real or anticipated health concern is described as the problem. For instance, decreased physical mobility
NANDA nursing diagnosis components
- Identification of the issue and its definition
- Concisely and clearly sums up the client's health status in a few words.
Qualifiers
- Deficient
- Inadequate in terms of quantity, quality, or degree; not enough
- Impaired
- Worsened, diminished, or ruined
- E (etiology)
- For example incisional pain
- S (symptoms or defining characteristics)
- Summarizes the identifying traits that serve as indicators of the health issue succinctly. An illustration would be limited twisting and placement.
- PES diagnostic statement
- Reduced physical mobility caused by incisional pain, as shown by constricted positioning and turning.
- Two part statements nursing diagnosis
- The problem statement or diagnostic label, which defines the client's response to a real, potential, and risky health concern or a wellness condition, makes up the first part. The etiology makes up the second element of a two-part nursing diagnostic. The linked cause or contributor to the issue is known as the etiology.
- Three part statements nursing diagnosis
- A three part statement can also be used to express the nursing diagnosis. This style, called PES, comprises the problem's origin, manifestations, and symptoms. The diagnostic label and the etiology are the first two parts, just like in the two-part statement. The defining qualities make up the third part (collected data that are also known as signs and symptoms, subjective and objective data, or clinical manifestations).
One, two, and three part nursing diagnosis statements are compared.
| one part statement | two part statement | three part statement |
|
Part 1: Wellness condition/state to be enhanced (no Related to, no etiology, and no defining characteristics) |
Part 1: Problem Related to Part 2: Etiology (no defining characteristics Part 1: Problem Related to |
Part 1: Problem Related to Part 2: Etiology The vile Part 3: Defining characteristics) |
Example of nursing diagnoses expressed in two and three part statements
| nursing diagnosis | two part statement | three part statement |
|
Feeding Deficit Self-Care |
Feeding Self-Care Deficit RT decreased strength and endurance | Feeding Self-Care Deficit RT decreased strength and endurance AEB inability to maintain fork in hand from plate to mouth |
| Ineffective Airway Clearance | Ineffective Airway Clearance RT Fatigue | Ineffective Airway Clearance RT Fatigue AEB dyspnea at rest |
| anxiety | Anxiety RT change in role functioning | Anxiety RT change in role functioning AEB insomnia, poor eye contact, and quivering voice |
| deficient knowledge | Deficient Knowledge RT misinterpretation of information | Deficient Knowledge RT misinterpretation of information AEB inaccurate return demon. stration of self-injection |
| spiritual distress | Spiritual Distress RT separation from religious ties | Spiritual Distress RT separation from religious ties AEB crying and withdrawal |
Writing a Nursing Diagnosis: Guidelines
- Instead of using nursing needs or interventions, describe the diagnosis in terms of the patient's response.
| Incorrect | Correct |
|
Needs suctioning because he has excessive High oral secretions. Offer bed pan frequently because of altered elimination pattern |
High risk for aspiration related to excessive oral secretion. Diarrhea related to food intolerance |
- Dentify the patient problem rather than the goal of care.
| Incorrect | Correct |
|
Patients' needs high protein diet related to potential alteration in nutrition. |
Imbalanced nutrition: less than body requirements related to inadequate protein intake. |
- Dentify the patient's problem rather than your problems with nursing care
| Incorrect | Correct |
|
Potential intravenous complications related to poor vascular access |
Risk for infection |
- Use "related to" rather than "due to" or "caused by" to connect the two parts of the statement
| Incorrect | Correct |
|
Altered sexuality patterns caused by change in body image. |
Altered sexually patterns related to change in body image. |
- Write the diagnosis in legally advisable terms.
| Incorrect | Correct |
|
High risk for trauma related to inadequately maintained skin traction. Recurrent angina related to insufficient medication
|
High risk for trauma related to hazards of skin traction. |
- Make professional rather than prejudicial judgments.
| Incorrect | Correct |
|
Altered parenting related bounding and child. to poor Impaired skin integrity related to poor I hygiene habits |
Altered parenting related prolonged to separation from child. Impaired skin integrity related to inadequate knowledge about perineal care |
- A diagnosis statement's first part should reflect human response and define outcomes; avoid reversing this part. The statement's second clause lists the relevant factors and suggests nursing interventions.
| Incorrect | Correct |
|
Confinement to home related to impaired social interaction. |
Impaired social interaction related to confinement to home. |
- Do not include medical diagnosis in the nursing diagnosis statement.
| Incorrect | Correct |
| Ineffective breathing patterns R/T/ emphysema. |
Ineffective secretions. breathing pattern R/T pattern retained |
- State the diagnosis clearly and concisely
| Incorrect | Correct |
| Fatigue related to dizziness | High risk for trauma related to dizziness. |
- Instead of focusing on the symptom in the first part of the statement, choose a NANDA-I diagnostic statement.
| Incorrect | Correct |
|
Withdrawn behavior related to inability to engage in satisfying personal relationships |
Social isolation related to inability to engage satisfying personal relationship. |
- Instead of relying solely on a single symptom, make a nursing diagnosis based on a group of distinguishing traits. For an issue to be identified, more than one symptom is required. For instance, "dyspnea" by itself does not necessarily result in a diagnosis. Dyspnea, shortness of breath, pain with inspiration, and a productive cough with thick secretions, however, are defining symptoms that result in the diagnosis of "ineffective breathing pattern due to increased airway secretions."
- Instead of focusing on a clinical symptom or a persistent issue that cannot be resolved with nursing intervention, identify a curable cause or risk factor. An individual with broken ribs will probably experience discomfort upon inhalation, have impaired chest excursion, and breathe more slowly and shallowly. Atelectasis may be visible in the affected area on an x-ray film.
| Incorrect | Correct |
| Ineffective breathing pattern related to shallow respirations |
Ineffective breathing pattern related to pain in chest |
- Instead than focusing on the treatment or diagnostic study itself, pinpoint the issue it caused.
| Incorrect | Correct |
|
Anxiety related to cardiac catherization |
Anxiety related to lack of knowledge about cardiac catherization |
- Instead of focusing on the equipment itself, note how the patient responded to it.
| Incorrect | Correct |
| Anxiety related to cardiac monitor | Deficient knowledge regarding the need for cardiac monitoring |
- By outlining the problem and its cause, avoid making a circular argument. Circular statements are non-specific and don't offer any direction for nursing care.
| Incorrect | Correct |
|
Impaired breathing pattern related to shallow breathing. |
Ineffective breathing pattern related to incisional pain. |
- In the diagnostic statement, just one patient issue should be mentioned. Every issue has distinctive predicted results. "Pain and anxiety associated to trouble in ambulating" is a nursing diagnostic that can refer to both "anxiety connected to difficulty in ambulating" and "limited physical movement related to pain in the right knee."
2015–2017 NANDA Nursing Diagnosis List
Domain 1. Health Promotion
- Class 1. Health awareness
- Deficient diversional activity
- Sedentary lifestyle
- Class 2. Health management
- Frail elderly syndrome
- Risk for frail elderly syndrome
- Deficient community
- Risk-prone health behavior
- Ineffective health maintenance
- Ineffective health management
- Readiness for enhanced health management
- Ineffective family health management
- Noncompliance
- Ineffective protection
Domain 2: Nutrition
- Class 1. Ingestion
- Insufficient breast milk
- Ineffective breastfeeding
- interrupted breastfeeding
- Readiness for enhanced breastfeeding
- Ineffective infant feeding pattern
- Imbalanced nutrition: less than body requirements
- Readiness for enhanced nutrition
- Obesity
- Overweight
- Risk for overweight
- Impaired swallowing
- Class 2. Digestion none at present time
- Class 3. Absorption none at present time
- Class 4. Metabolism
- Risk for unstable blood glucose level
- Neonatal jaundice
- Risk for neonatal jaundice
- Risk for impaired liver function
- Class 5. Hydration
- Risk for electrolyte imbalance
- Readiness for enhanced fluid balance
- Deficient fluid volume
- Risk for deficient fluid volume
- Excess fluid volume
- Risk for imbalanced fluid volume
Domain 3: Elimination and exchange
- Class 1. Urinary function
- Impaired urinary elimination
- Readiness for enhanced urinary elimination
- Functional urinary incontinence
- Overflow urinary incontinence
- Reflex urinary incontinence
- Stress urinary incontinence
- Urge urinary incontinence
- Risk for urge urinary incontinence
- Urinary retention
- Class 2. Gastrointestinal function
- Constipation
- Risk for constipation
- Chronic functional constipation
- Risk for chronic functional constipation
- Perceived constipation
- Diarrhea
- Dysfunctional gastrointestinal motility
- Risk for dysfunctional gastrointestinal motility
- Bowel incontinence
- Class 3. Integumentary function none at this time
- Class 4. Respiratory function
- Impaired gas exchange
Domain 4: Activity/rest
- Class 1. Sleep/rest
- Insomnia
- Sleep deprivation
- Readiness for enhanced sleep
- Disturbed sleep pattern
- Class 2. Activity/exercise
- Risk for disuse syndrome
- Impaired bed mobility
- proscut time
- Impaired physical mobility
- Impaired wheelchair mobility
- Impaired sitting
- Impaired standing
- Impaired transfer ability
- Impaired walking
- Class 3. Energy balance
- Fatigue
- Wandering
- Class 4. Cardiovascular/pulmonary responses
- Activity intolerance
- Risk for activity intolerance
- Ineffective breathing pattern
- Decreased cardiac output
- Risk for decreased cardiac output
- Risk for impaired cardiovascular function
- Risk for ineffective gastrointestinal perfusion
- Risk for ineffective renal perfusion
- Impaired spontaneous ventilation
- Risk for decreased cardiac tissue perfusion
- Risk for ineffective cerebral tissue perfusion
- Ineffective peripheral tissue perfusion
- Risk for ineffective peripheral tissue perfusion
- Dysfunctional ventilatory weaning response
- Class 5. Self-care
- Impaired home maintenance
- Bathing self-care deficit
- Dressing self-care deficit Feeding self-care deficit
- Toileting self-care deficit
- Readiness for enhanced self-care
- Self-neglect
Domain 5: Perception/Cognition
- Class 1. Attention
- Unilateral neglect
- Class 2. Orientation\
- None at this time
- Class 3. Sensation/perception
- None at this time
- Class 4. Cognition
- Acute confusion
- Risk for acute confusion
- Chronic confusion
- Labile emotional control
- Ineffective impulse control
- Deficient knowledge
- Readiness for enhanced knowledge
- Impaired memory
- Class 5. Communication
- Readiness for enhanced communication
- Impaired verbal communication
Domain 6: Self-Perception
- Class 1. Self-concept
- Readiness for enhanced hope
- Hopelessness
- Risk for compromised human dignity
- Disturbed personal identity
- Risk for disturbed personal identity
- Readiness for enhanced self-concept
- Class 2. Self-esteem
- Chronic low self-esteem
- Risk for chronic low self-esteem
- Situational low self-esteem
- Risk for situational low self-esteem
- Class 3. Body image
- Disturbed body image
Domain 7: Role relationships
- Class 1. Caregiving roles
- Caregiver role strain
- Risk for caregiver role strain
- Impaired parenting
- Readiness for enhanced parenting
- Risk for impaired parenting
- Class 2. Family relationships
- Risk for impaired attachment
- Dysfunctional family processes
- Interrupted family processes
- Readiness for enhanced family processes
- Class 3. Role performance
- Ineffective relationship
- Readiness for enhanced relationship
- Risk for ineffective relationship
- Parental role conflict
- Ineffective role performancety
- Impaired social interaction vadrome
Domain 8: Sexuality
- Class 1. Sexual identity none at present time
- Class 2. Sexual function
- Sexual dysfunction
- Ineffective sexuality pattern
- Class 3. Reproduction
- Ineffective childbearing process
- Readiness for enhanced childbearing process
- Risk for ineffective childbearing process
- Risk for disturbed maternal-fetal dyad
Domain 9: Coping/stress tolerance
- Class 1. Post-trauma responses Post-trauma syndrome
- Risk for post-trauma syndrome
- Rape-trauma syndrome
- Relocation stress syndrome
- Risk for relocation stress syndrome minist
- Class 2. Coping responses
- Ineffective activity planning
- Risk for ineffective activity planning
- Anxiety
- Defensive coping
- Ineffective coping
- Readiness for enhanced coping
- Ineffective community coping
- Readiness for enhanced community coping
- Compromised family coping
- Disabled family coping
- Readiness for enhanced family coping
- Death anxiety
- Ineffective denial
- Fear
- Grieving
- Complicated grieving
- Risk for complicated grieving
- Impaired mood regulation
- Readiness for enhanced power
- Powerlessness
- Risk for powerlessness
- Impaired resilience
- Readiness for enhanced resilience
- Risk for impaired resilience
- Chronic sorrow
- Stress overload
- Class 3. Neurobehavioral stress
- Decreased intracranial adaptive capacity
- Autonomic dysreflexia
- Risk for autonomic dysreflexia
- Disorganized infant behavior
- Readiness for enhanced organized infant behavior
- Risk for disorganized infant behavior
Domain 10: Life Principles
- Class 1. Values none at this time
- Class 2. Beliefs
- Readiness for enhanced spiritual well-being
- Class 3. Value/belief/action congruence
- Readiness for enhanced decision-making
- Decisional conflict
- Impaired emancipated decision-making
- Readiness for enhanced emancipated
- Decision-making
- Risk for impaired emancipated decision-making morb
- Moral distress
- Impaired religiosity
- Readiness for enhanced religiosity
- Risk for impaired religiosity
- Spiritual distress
- Risk for spiritual distress
Domain 11: Safety/Protection
- Class 1. Infection
- Risk for infection
- Class 2. Physical injury
- Ineffective airway clearance
- Risk for aspiration
- Risk for bleeding
- Risk for dry eye
- Risk for falls risk for injury
- Risk for corneal injury
- Risk for perioperative positioning injury
- Risk for thermal injury
- Risk for urinary tract injury
- Impaired dentition
- Impaired oral mucous membrane
- Risk for impaired oral mucous membrane
- Risk for peripheral neurovascular dysfunction
- Risk for pressure ulcer
- Risk for shock
- Impaired skin integrity
- Risk for impaired skin integrity
- Risk for sudden infant death syndrome
- Risk for suffocation Delayed surgical recovery
- Risk for delayed surgical recovery
- Impaired tissue integrity
- Risk for impaired tissue integrity
- Risk for trauma
- Risk for vascular trauma
- Class 3. Violence
- Risk for other-directed violence
- Risk for self-directed violence
- Self-mutilation
- Risk for self-mutilation
- Risk for suicide
- Class 4. Environmental hazards
- Contamination
- Risk for contamination
- Risk for poisoning
- Class 5. Defensive processes
- Risk for adverse reaction to iodinated contrast media
- Risk for allergy response
- Latex allergy response
- Risk for latex allergy response
- Class 6. Thermoregulation
- Risk for imbalanced body temperature
- Hyperthermia
- Hypothermia
- Risk for hypothermia
- Risk for perioperative hypothermia
- Ineffective thermoregulation
Domain 12: Comfort
- Class 1. Physical comfort
- Impaired comfort
- Readiness for enhanced comfort
- Nausea
- Acute pain
- Chronic pain
- Labor pain
- Grieving
- Chronic pain syndrome
- Class 2. Environmental comfort
- Impaired comfort
- Readiness for enhanced comfort
- Class 3. Social comfort
- Impaired comfort
- Readiness for enhanced
- Comfort Risk for loneliness
- Social isolation
Domain 13: Growth/development
- Class 1. Growth
- Risk for disproportionate growth
- Class 2. Development
- Risk for delayed development
Things to remember title
© 2021 Saralmind. All Rights Reserved.
 Login with google
Login with google